How do you treat tumor lysis syndrome
In general, treatment of TLS consists of intensive hydration, stimulation of diuresis, and, more specifically, in the use of allopurinol and rasburicase.
Is allopurinol used for tumor lysis syndrome?
It is usually given orally at 600 mg daily for prophylaxis and 600-900 mg daily (up to a maximum of 500 mg/m2 daily) for treatment of tumor lysis syndrome. Patients unable to take oral medications can be given IV allopurinol.
Is tumor lysis syndrome an emergency?
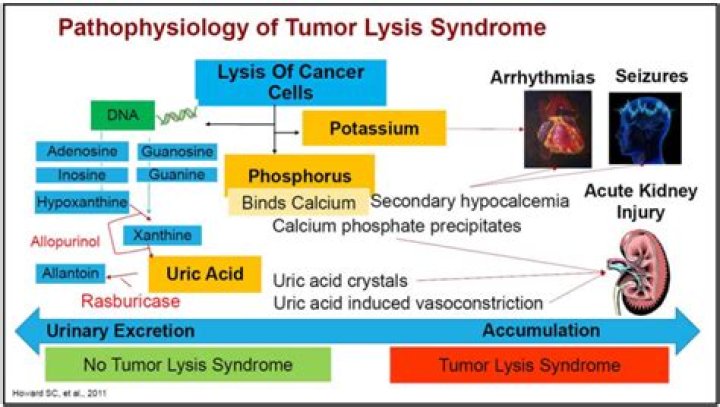
Tumor Lysis Syndrome (TLS) is an oncologic emergency due to massive tumor cell lysis, characterized by metabolic abnormalities that can lead to renal failure, seizures, and dysrhythmia.
What happens with tumor lysis syndrome?
Tumor lysis syndrome (TLS) is a condition that occurs when a large number of cancer cells die within a short period, releasing their contents in to the blood.What medication prevents tumor lysis syndrome?
Febuxostat (Uloric) is a novel xanthine oxidase inhibitor that does not appear to have the hypersensitivity profile of allopurinol. In addition, this agent does not require dosing modification for renal impairment. Initial studies suggested that febuxostat is effective and safe for preventing tumor lysis syndrome.
How can you prevent and manage tumor lysis syndrome?
The most important treatment for TLS is prevention. The mainstays of TLS prevention include aggressive hydration, control of hyperuricemia with allopurinol and rasburicase treatment, and close monitoring of electrolyte abnormalities.
How is hyperphosphatemia treated in tumor lysis syndrome?
Treatment of hyperphosphatemia reduces dietary phosphate intake and includes phosphate binders such as aluminum hydroxide and aluminum carbonate. When recurrent hypocalcemia is present, a continuous intravenous infusion of calcium gluconate can be initiated.
Which of the following symptoms might a patient experience with TLS?
Clinical symptoms include hyperkalemia, hyperphosphatemia, hypocalcemia, nausea, vomiting, diarrhea, anorexia, lethargy, hematuria, muscle cramps, syncopy, heart failure, and cardiac dysthymias.Can you survive tumor lysis syndrome?
Prognosis in tumor lysis syndrome depends on the underlying malignancy characteristics. In patients with a hematologic malignancy, the mortality rate for tumor lysis syndrome is approximately 15%. The reported mortality of tumor lysis syndrome in patients with solid malignancies is reported at 36%.
Can you have tumor lysis syndrome without chemo?Tumor lysis syndrome (TLS) presenting in absence of chemotherapy is a rare occurrence. One of the true oncological emergencies, it can lead to significant morbidity and mortality. TLS is a phenomena usually associated with tumor cell death after treatment.
Article first time published onWhich treatment strategy increases the risk for developing tumor lysis syndrome?
The risk is particularly high when patients have very high serum phosphorus levels and require intravenous calcium to treat symptomatic hypocalcemia. High solute concentration, low solubility, and slow urine flow make crystallization more likely and therefore increase the risk for tumor lysis syndrome.
What is Rasburicase?
Rasburicase injection is used to treat high levels of uric acid (a natural substance that builds up in the blood as tumors break down) in people with certain types of cancer who are being treated with chemotherapy medications. Rasburicase injection is in a class of medications called enzymes.
Which drugs are used in the treatment of hyperkalemia high serum potassium level due to tumor lysis syndrome?
Sodium polystyrene sulfonate is an exchange resin that can be used to treat mild to moderate hyperkalemia. Each milliequivalent of potassium is exchanged for 1 mEq of sodium. Agents to treat hyperphosphatemia are also used.
Which of the following is a strategy to prevent tumor lysis syndrome for a patient that is at intermediate risk?
hydration is the key prevention strategy for all patients at low, intermediate, or high risk for TLS. Hydration, and the subsequent increase in urinary output, minimizes the risk of uric acid or calcium phosphate precipitation in the renal tubules.
When do you give TLS prophylaxis?
Therefore, it is recommended that the treatment should be started 2–3 days before chemotherapy and continued at least for 10–14 days or until the signs of massive tumor lysis are absent [27, 73]. Typically, the drug is given orally at a dose of 600–800 mg daily; if necessary, it can also be given intravenously.
How do you fix hyperphosphatemia?
- I. Diet: restricting dietary phosphate intake.
- II. Enhancing elimination: removing phosphate with adequate dialysis.
- III. Minimising phosphate absorption: reducing intestinal absorption using phosphate binders.
When do you give Rasburicase for tumor lysis syndrome?
The first dose of rasburicase should be administered 4 to 24 hours before starting chemotherapy. Rasburicase is given as an intravenous infusion over 30 minutes and should not be given as a bolus infusion (4).
What is Rasburicase and what is its role in the mitigation of TLS?
Rasburicase, a recombinant urate oxidase enzyme, is a new agent indicated in the treatment or prophylaxis of hyperuricemia in pediatric patients with cancer who are at high risk for TLS.
What are the primary prophylactic strategies for TLS?
The best management of TLS is prevention. Prevention strategies include hydration and prophylactic rasburicase in high-risk patients, hydration plus allopurinol or rasburicase for intermediate-risk patients, and close monitoring for low-risk patients.
How does tumor lysis cause Aki?
High levels of both uric acid and phosphate render patients with the tumor lysis syndrome at particularly high risk for crystal-associated acute kidney injury, because uric acid precipitates readily in the presence of calcium phosphate, and calcium phosphate precipitates readily in the presence of uric acid.
Why is there hyperphosphatemia in tumor lysis syndrome?
Hyperphosphatemia is another electrolyte imbalance associated with tumor lysis syndrome. The nucleic acid has a phosphate group, and the breakdown of the tumorous cell will lead to the release of a significant amount of phosphorus into the bloodstream. Most of the phosphorus is renally excreted.
Is tumor lysis syndrome good or bad?
The syndrome characterized by these metabolic derangements is known as tumor lysis syndrome (TLS). TLS can cause life-threatening conditions and even death unless appropriately and immediately treated.
Is Tumour lysis syndrome painful?
Symptoms of tumour lysis syndrome may be mild at first. They get worse as the levels of abnormal substances in the blood increase.
What are the complications of tumor lysis syndrome?
Potential complications of tumor lysis syndrome include uremia and oliguric renal failure due to tubule precipitation of uric acid, calcium phosphate, or hypoxanthine. Severe electrolyte disturbances, such as hyperkalemia and hypocalcemia, predispose patients to cardiac arrhythmia and seizures.
What is spontaneous tumor lysis syndrome?
Spontaneous tumor lysis syndrome is a rare oncological emergency associated with multiorgan failure. It is characterized by an elevation of uric acid, hyperphosphatemia, hypocalcemia, hyperkalemia and renal failure in the setting of no active chemotherapy as a result of lysis of massive tumor burden.
Does chemo cause tumor necrosis?
After chemotherapy, regardless of tumor volume and location, control group tumors showed an increase in the tumor necrosis of approximately 50 %. Conclusion: In chemotherapy era, the extent of spontaneous necrosis has no relation with survival.
How do you know when a tumor is dying?
- Worsening weakness and exhaustion.
- A need to sleep much of the time, often spending most of the day in bed or resting.
- Weight loss and muscle thinning or loss.
- Minimal or no appetite and difficulty eating or swallowing fluids.
- Decreased ability to talk and concentrate.
Do tumors bleed when they shrink?
Tumor bleed is commonly seen in locally progressive tumors, which have directly infiltrated blood vessels. However, tumor bleed secondary to rapid shrinkage has not been reported previously. We report on a patient who had a torrential bleed after initiation of multi-agent chemotherapy.
Does Chemo increase uric acid?
Certain cancers, or chemotherapy agents may cause an increased turnover rate of cell death. This is usually due to chemotherapy, but high uric acid levels can occur before chemotherapy is administered. After chemotherapy, there is often a rapid amount of cellular destruction, and tumor lysis syndrome may occur.
How is superior vena cava syndrome treated?
The main treatment for SVCS is to treat the cancer that is causing it with chemotherapy or radiotherapy. However, other things can be done to alleviate the symptoms. Your doctor might prescribe corticosteroids to reduce swelling or diuretics to remove excess fluid from your body by increasing urination.
Why is LDH elevated in tumor lysis syndrome?
An increase in lactate dehydrogenase (LDH) is typically seen in patients with TLS, probably because of anaerobic glucose metabolism. However, the elevation of LDH is not included in the laboratory definition of LDH and it is important to note that LDH is a very sensitive but quite nonspecific marker for TLS.